|
| How's my running gait? |
I saw a patient yesterday who was training for the upcoming Singapore marathon. He started having knee and heel pain after doing a long run of 22 km over the weekend. Upon assessment, he definitely demonstrated a greater contralateral (or opposite) pelvic drop (CPD), indicating
Gluteus Medius muscle weakness.
 |
| Picture A- Injured runner with CPD and right hip adduction |
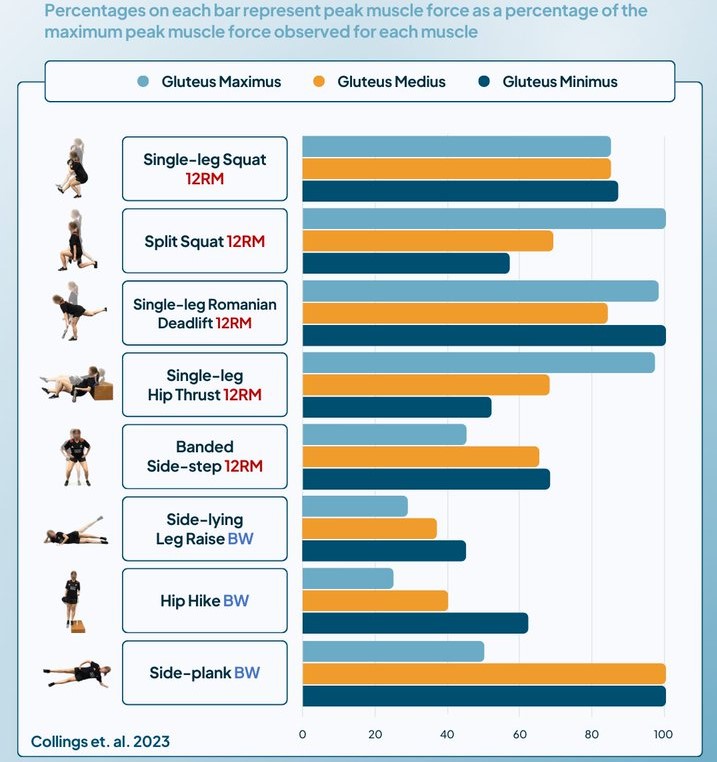
Last week we discussed whether doing
clam shell exercises was still relevant for someone with
Gluteus Medius muscle weakness. Turn's out that this week's post is related to that.
The referenced study (Bramah et al, 2018) investigated and identified certain faulty running gait patterns that contribute to running injuries. In all, 108 runners were studied, including 72 injured runners and 36 healthy runners in the control group matched for age, height and weight.
None of the injured runners received any prior treatment for their injury. Those with an increase with more than 30 percent in training volume were also excluded from the study. The control group of runners ran at least 30 miles (or 48 km) a week.
The injuries the injured runners had were patella femoral pain (
PFP),
Iliotibial Band Syndrome (ITBS), Medial Tibial Stress Syndrome (MTSS or
shin splints) and
Achilles Tendinopathy (AT). The injuries were selected as they are most prevalent among runners.
All the injured runners showed a greater contralateral (or opposite) pelvic drop (CPD), demonstrating Gluteus Medius muscle weakness. They had a more extended knee and dorsiflexed ankle (heel striking) at initial contact and a forward trunk lean at the midstance phase of running. These patterns were consistent across each of the four injured groups.
 |
| Contralateral pelvic drop |
CPD was found to be the most important variable predicting whether the study participants were healthy or injured. For every 1 degree increase in pelvic drop, there was a 80 percent increase in the odds of getting injured.
 |
| Injured runner (L) heel striking, forward trunk lean vs normal |
Those who had more knee extension makes the patella (kneecap) more vulnerable to lateral tilting and displacement. This may affect knee joint contact areas and increase stress when the foot strikes the ground. If a runner
heel strikes with the knee extended, their center of mass is further away from their foot. This leads to an increase in knee joint loading and a increase "braking" forces (imagine applying brakes on while you're running).
Those with a forward trunk lean may have weakness around the back and gluteal muscles as shown by previous studies. The injured runners with
PFP and
ITB problems had more hip adduction than other runners. More
female runners were also found to more hip adduction compared to male runners.
So make sure your
Gluteus Medius muscles are
strong enough so that you will be less likely to have a running injury.
References
Bramah C, Preece SJ Nimh G et al (2018). Is There A Pathological Gait Associated With Common Soft Tissue Running Injuries? AJSM. 46(12): 3023-3031. DOI: 10.1177/0363546518793657
Lessi GC, Dos Santos AF et al (2017). Effects Of Fatigue On Lower Limb, Pelvis And Trunk Kinematics And Muscle Activation. J Electrom Kinesiol. 32: 9-14