

However since restrictions were lifted for Covid-19, the younger members of our team decided we should go bowling.


Mark your calenders for the next team building event on June 3rd. Stay tuned.

Mark your calenders for the next team building event on June 3rd. Stay tuned.
 |
| Ice baths for recovery |
Can you see the error with this conclusion? Neumann and colleagues (2021), sugests that sports scientists may inadvertently be making errors like this frequently. Their research studied the relationship between training load and recovery. If you're into endurance sports, you know recovery is really crucial.
When you train more, your fitness improves, however, it also increases your chances of injury and burnout. This has led to all sorts of research to investigate how we handle different training loads and how quickly we recover so that we can train harder without breaking down.
So, is there a link between training load and recovery? Is it possible to measure training load and subsequent recovery in a large group of people and use those results to recommend or predict how you and I or any individual would respond?
Neumann and colleagues (2020) studied footballers from a top Dutch football league club, over 2 seasons. Daily training and recovery data were collected from footballers of their under-17, under-19 and under-23 teams.
The most basic question to address is if total training load in a workout affect how recovered the footballers feel before the next day's training session? This is done in 2 ways.

For each individual analysis, you monitor every pair of workout/ recovery scores for each individual over the course of the data. This data is then averaged.
If both group and individual data produce identical results, then the training and recovery is ergodic, meaning the results of the group studies can be applied to individuals (like you and I). If results aren't identical then oops.....
Well, sure enough, the group and individual analyses produced different results. The correlations between training load and recovery did not match up. training loads varied far more for a given individual footballer over time than they did between individual footballers on a given day. How a bunch of people respond to a single workout session does not always tell how you respond to a series of workouts.
I recall when running cross country in secondary school how all of us in the school team were given the same workout session and each of us responded differently.
You must be wondering now if all the previous research done on training and on large groups apply to you, or whether they are invalid. Researchers use randomized placebo controlled trials to normalise the effects of individual variation. They also report individual results to group averages.
Read and understand the recommendations from researchers to improve your personal training/ performance and recovery. But bear in mind that we are all an experiment of one (or n = 1). Age is also a confounder. What hurts now after a certain workout did not hurt when I was 28.
Reference
Neumann ND, Yperen NWV, Brauers JJ et al (2021). Nonergodicity In Load And Recovery: Group Results Do Not Generalize To Individuals. Int J Sp Physiol Perform. 17(3): 391-399. DOI: 10.1123/ijspp.2021-0126

I thought it's common knowledge by now that just one static stretch of 30 seconds can reduce your maximum strength. You're more likely to get injured if you do static stretching before exercising.
Maybe that physiotherapist is not alone. An article published in 2020 found that 80 percent of 605 personal trainers surveyed in the United States of America still prescribed traditional static stretching to their clients.
Static stretching is prescribed to help static flexibility. Some readers will recall doing the sit-and-reach test in the NAPFA test in our schools. This is done sitting on the floor with legs out straight and they measure how far beyond your heels you can reach. Best way to improve static flexibility? To do more static stretching. You can go to the end of your available range and hold that for say, 10 seconds and repeat.
If you read that article (Nuzzo, 2020), having good flexibility will not help you live longer. It does not help prevent falls.
Good static flexibility also does not help prevent injuries. This topic has been the studied widely, a few studies have found that there are some benefits, while a few other studies have found that being too flexible is associated with injury. Most do not seem to make much difference.
Static flexibility is not associated with non sports related problems like low back pain.
Most importantly for the readers of this blog, having better static flexibility does not improve your sporting performance. Unless your sport requires a certain range like in gymnastics or if you are trying to become a ballerina. Donaben, our champion cyclist will tell you that time trialling on a bike will require some flexibility to hold that aerodynamic tuck and still pedal with power. The rest of us? Probably not.
If you are a runner, you are unlikely to get injured if you cannot touch your toes. A study found that amongst elite runners (with an average VO2 max of 73 mL/kg/min), the runners who were the least flexible (in the sit-and-reach test) were the most economical runners (better running economy). This suggests that being less flexible is better as this allows your legs to store and return energy (like a coiled spring) with each running stride (Jones, 2002)
So take note that static flexibility is not that important, unless your specific sport requires it. Stretching before, during or after a workout does not prevent subsequent muscle soreness. It does not reduce inury risk either (Herbert et al, 2011).
So what do you do to warm up before your exercise if you do not stretch? The goal of warming up is to physically warm your muscles to make them more pliable as well as get your heart rate up to be ready to deliver oxygen to your working muscles.
Before my run, I'll ride a stationary bike for 10 minutes or just run the first kilometer real slow before picking up the pace. If you're playing badminton or tennis, I'll suggest some lunges, side to side movements, i.e. sport specific movements that you may use while playing.
Want to improve your range of motion? Try strength training instead.
References
Jones AM (2002). Running Economy Is NegativelyRelated To Sit-and-reach Test Performance In International-standard Distamce Runners. Int J Sp Med. 23(1): 40-43. DOI: 10.1055/s-2002-19271
Nuzzo JL (2020). The Case For Retiring Flexibility As A Major Component Of Physical Fitness. Sports Med. 50(5): 853-870. DOI: 10.1007/s40279-019-01248-w
Herbert RD, Noronha MD and Kamoer SJ (2011). Stretching To Prevent Or Reduce Muscle Soreness After Exercise. Cochrane Reviews. DOI: 10.1002/14651858.CD004577.pub3
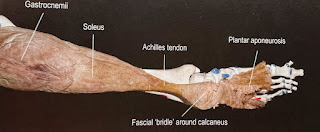
Trained runners have been found to have a thicker Achilles tendon, stiffer and better structure compared to novice runners. A longer, stiffer tendon stores more energy and releases that energy when you push off with each step. It has also been speculated that the dominance of international running races by Kenyan runners are due to their long and springy Achilles tendon (Tawa and Louw, 2018).
Can you then train your tendons? Consider the following study. 40 pairs of identical twins were asked about their physical activity and sports habits to determine how active they were. Researchers then measured the stiffness of their Achilles tendons.
Results show that when one twin is active and the other inactive, the active twins have tendons 28 percent stiffer. Since identical twins start with identical genes, this shows that long term training can change the structure of the Achilles. It also fits in with previous studies that trained runners have thicker and stiffer tendons. These runners were not elite runners so you don't need excessive training levels to change your tendons. But these runners have been running for an average of 15 years, so there's plenty of time for change to occur.
Another point to note from the study. Those who did activities that involve an aerial phase with both feet off the ground (running, basketball or tennis etc) had a stiffer TA compared to those with no aerial phase (cycling, walking and swimming). This suggests that jumping and landing may hold clues to getting your Achilles tendon stiffer and stronger.
Tendons may be slow to heal and adapt to load, but for those of you who run, surely this is an incentive to keep on running. Those who play football, basketball or tennis, please carry on too.
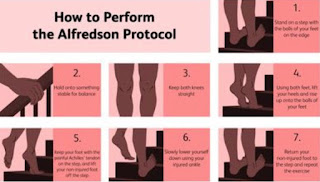
Currently, when you visit your current healthcare provider for treatment, most will just recommend the Alfredson protocol (up to 180 eccentric heel drops a day) to get your Achilles tendon better. That you can do yourself (picture below).
In our clinics, after we assess you thoroughly, we mostly use our hands to treat what we find, no ultrasound, no orthotics, no shockwave (ESWT), no electrotherapy. And we get very good results. We DO NOT get you to do exercises DURING the time you have with us. We do treatment that you cannot do yourself.
Previously, I've written that there is some evidence that gelatin (or jell-o) can help tendons heal. Perhaps that is an area you may also want to explore? And do take note that some antibiotic medications can damage your tendons.
References
Sichting F, Kram NC and Legerlotz K (2022). An Identical Twin Study On Human Achilles Tendon Adaptation: Egular Recreatinal Exercise At Comparatively Low Intensities Can Increase Tendon Stiffness. Front. Physiol. DOI: 10.3389/fphys.2021.777403
Tawa N and Louw Q (2018). Biomechanical Factors Associated With Running Economy And The Performance Of Elite Kentyan Distance Runners: A Systematic Review. J Body Mvt Ther. DOI: 10.1106/j.bmt.2017.11.004

The public pool we were using is only opened for lap swimming now. We are very grateful to The Ripple Club. It was with their help that we got access to a pool for our post-op patients today.
 |
| They are all surrendering.... |
For our sessions, the pool is usually 1.8 metres deep. The patients use an aqua running belt to keep them afloat.
One patient had her hip labrum repaired recently while another (a triathlete) had an OCD bone fragment removed surgically. I often include aqua running techniques (or deep water running) to produce a training effect for them since they definitely cannot run on land yet.
If done correctly, the arms, shoulders, lower limbs and abdominal muscles are involved. For those who cannot take too much impact, this is a very good alternative since water is 773 times more resistant than air. The harder you move your arms or legs, the more drag force or resistance you encounter.
 |
| Sculling with aqua belts off |



