|
| Back view of L calcaneus |
Yes, I still ran twice a week even though I had some pain while running. Some of that same pain came back during our recent holiday in Japan. I did not cycle nor run during the trip but did some skipping for the first few days of our trip.

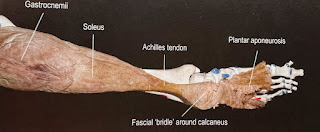
The Achilles tendon is the largest/ longest tendon in the human body and is formed when the medial (inner) and lateral (outer) parts of the gastrocnemius and soleus muscles merges.
The authors dissected 12 fresh frozen leg specimens to find where the Achilles tendon inserts (or finishes) on the calcaneus in relation to their corresponding muscles. They also examined 10 embalmed specimens to confirm an observation on the retrocalcaneal bursa. A bursa is fluid filled sac/ pouch that acts as a cushion and gliding surface to reduce friction.
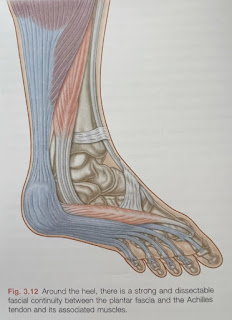
The superficial part of where the Achilles tendon finishes is where the medial head of the gastrocnemius muscle attaches (in light blue) on to the lower facet of the calcaneus. The authors (like previous studies) found evidence that tendon of the medial gastrocnemius forming the superficial part of the Achilles tendon is continous with the plantar fascia. Like I written before, in order to get the Achilles tendon better, you need to treat the plantar fascia and vice versa.
The deep part of where the Achilles tendon finishes is where the soleus muscle attaches on the inner part of the middle facet of the calacneus, while the lateral head of the gastrocnemius muscle attaches (in red) on to the outside part of the middle facet of the calacneus.
In the space between the calcaneus and the Achilles tendon, a distinct 2 chamber bursa was present in 15 out of 22 examined specimens (9 out of 12 fresh frozen specimens and 6 of the 10 embalmed). The smaller shallow medial chamber is located in front of the soleus tendon whereas the lateral chamber is in front of the lateral head of gastrocnemius tendon.
Here's what amazes me. From the dissections, the authors found that the Achilles tendon rotates as it goes down the leg. Meaning the fibers from the medial gastrocnemius head forms the back aspect of the tendon while the anterior part of the tendon is formed by the lateral gastrocnemius head and soleus muscles.
This article was helpful as it helped me pinpoint exactly where my problem was and most importantly it helped deepen my understanding of the function of each muscular, connective tissue part of the gastrocnemius, soleus and the Achilles tendon and their clinical relevance in the treatment of Achilles and plantar fascia problems.
So, if you are still having problems with your Achilles tendon and it does not seem to be getting better, show your healthcare practitioner the topmost picture so they know exactly which part to take note of. If they don't you can always come to our clinics.
Reference
Ballal MS, Walker CR and Molloy AP (2014). The Anatomical Footprint Of The Achilles Tendon: A Caderveric Study. Bone Joint J. 96B: 1344-1348. DOI: 10.10=302/0301-620X.96B10.33771